

Arthritis of the shoulder
What is shoulder arthritis?
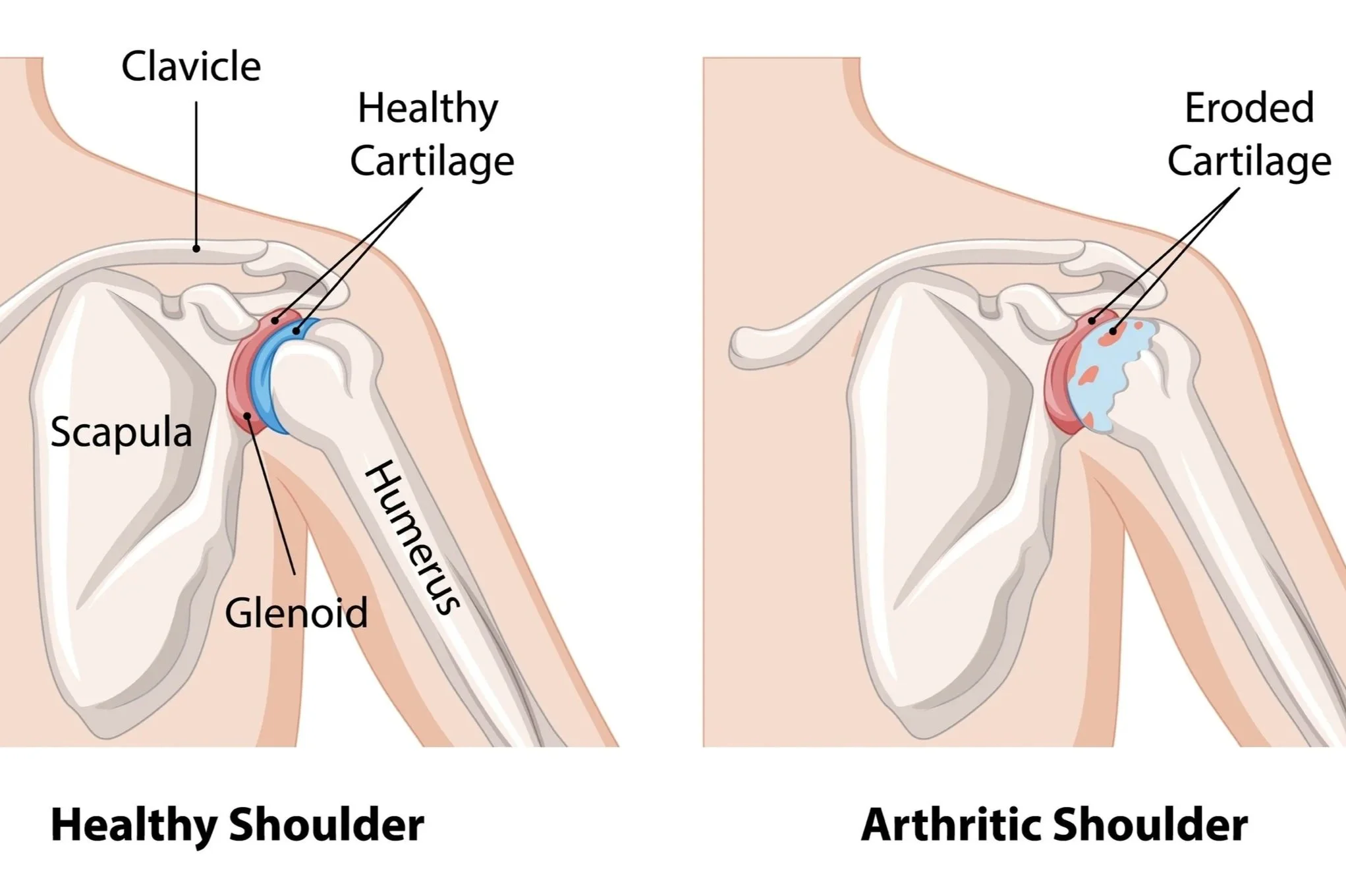
Arthritis is defined as inflammation of one or more joints. It occurs when the cartilage between the joint surfaces breaks down, meaning there is no longer a smooth gliding surface for the bones to move against each other. As the cartilage wears away, the bones begin to rub together, leading to pain, stiffness, swelling, weakness, and loss of movement.
The shoulder contains two main joints that can be affected by arthritis — the glenohumeral joint (the main ball-and-socket joint) and the acromioclavicular (AC) joint on the top of the shoulder.
The most common forms of shoulder arthritis are osteoarthritis, rheumatoid arthritis, post-traumatic arthritis, and rotator cuff tear arthropathy.
Osteoarthritis is the most common “wear-and-tear” form of arthritis. It develops gradually over time as the cartilage in the joint wears down with age and use. It is more common in people over the age of 50 and may affect either the main shoulder joint or the AC joint.
Rheumatoid arthritis is an autoimmune condition where the body’s immune system attacks the lining of the joints. It commonly affects both shoulders and can lead to pain, swelling, stiffness, and progressive joint damage if left untreated.
Post-traumatic arthritis can develop after a previous shoulder injury such as a fracture, dislocation, or significant ligament injury. Even when injuries heal well, damage to the joint surface can increase the risk of arthritis developing later in life.
Rotator cuff tear arthropathy is a type of shoulder arthritis that develops after a large or long-standing rotator cuff tear. When the rotator cuff tendons no longer function properly, the shoulder can become unstable, causing abnormal wear within the joint and resulting in pain, weakness, and arthritis.
How do I know if I have arthritis of the shoulder?
Symptoms of shoulder arthritis usually develop gradually and may worsen over time.
The most common symptom is pain. The location of the pain often depends on which part of the shoulder is affected. Arthritis in the main shoulder joint typically causes pain deep within the shoulder or toward the back of the joint, while arthritis in the AC joint usually causes pain on the top of the shoulder.
Other common symptoms include:
Stiffness and reduced movement
Difficulty lifting the arm
Pain reaching overhead or behind the back
Grinding, clicking, or crunching sensations
Weakness in the shoulder
Pain at night or difficulty sleeping
As the arthritis progresses, everyday activities such as brushing your hair, dressing, lifting objects, or reaching into cupboards may become increasingly difficult.
Patients with rotator cuff tear arthropathy may also notice significant weakness and difficulty lifting the arm away from the body.
How Ben can help?
Diagnosing shoulder arthritis
Ben will typically be able to diagnose shoulder arthritis and/or assess whether surgical intervention is required by examining the shoulder joint and assessing range of motion, tenderness, swelling, muscle weakness and/or joint instability. Furthermore, he will order X-rays to learn more about the exact location and severity of your arthritis. In some cases, further imaging such as an MRI or CT scan may be recommended to assess the cartilage, rotator cuff tendons, or surrounding bone in more detail. Blood tests may also be necessary to determine which type of arthritis you have.
Treating shoulder arthritis
Non-surgical treatment
There are a myriad of non-surgical treatments for shoulder arthritis that will normally be recommended before surgical intervention. Usually these will be recommended by your GP and only once these treatments have been exhausted will a referral to Ben be necessary. These options include:
Medication
Activity modification
Heat or ice therapy
Injections
Specific physiotherapy and strengthening exercises
For inflammatory forms of arthritis such as rheumatoid arthritis, specialised medications prescribed by a rheumatologist may help slow disease progression and protect the joints.
The non-surgical treatment option/s recommended to you will be based on:
How far the arthritis has progressed
Your age, activity level and other medical conditions
Whether your dominant or non-dominant shoulder is affected
Your personal goals, home support structure, and ability to understand the treatment and comply with a therapy program
Surgical treatment
Ben will usually recommend surgery if non-surgical treatments have failed to provide pain relief. Surgery will be different for every patient and will depend on the type of arthritis, the severity of joint damage, the condition of the rotator cuff tendons, and your age and activity level. The tailored surgical approach will be explained to you by Ben during your consult.
There are a number of surgical options:
Keyhole Surgery (Arthroscopic Debridement) - This type of surgery is commonly used in the earlier stages of shoulder arthritis. During this minimally invasive procedure, a small camera and specialised instruments are inserted through tiny incisions around the shoulder. The surgery is used to remove loose cartilage fragments, clean inflamed tissue, and trim painful bone spurs within the joint.
Although this procedure may improve symptoms, it does not reverse arthritis, and relief may be temporary if the arthritis continues to progress.
Distal Clavicle Excision (AC Joint Surgery) - For arthritis affecting the AC joint on the top of the shoulder, a distal clavicle excision may be recommended.
During this procedure, a small portion of the end of the collarbone is removed to prevent the arthritic bones from rubbing against each other. Over time, scar tissue forms in the space, which helps reduce pain while preserving shoulder movement.
This surgery may be performed arthroscopically or through a small open incision.
Hemiarthroplasty (Partial Shoulder Replacement) - A hemiarthroplasty involves replacing only the ball portion of the shoulder joint (the humeral head) with an artificial metal component.
Ben will usually recommend this surgery when the socket surface is still relatively preserved or in certain fracture situations. It is less commonly performed today than total shoulder replacement.
Total Shoulder Replacement (Total Shoulder Arthroplasty) - Total shoulder replacement is commonly performed for advanced arthritis when both sides of the joint are damaged but the rotator cuff tendons remain functional.
During the procedure, the damaged ball-and-socket surfaces are removed and replaced with artificial components made from metal and plastic. The metal ball replaces the humeral head, while a smooth plastic component is placed into the socket.
This operation aims to reduce pain, improve movement, and restore shoulder function. Many patients experience significant pain relief and improved quality of life following surgery
Reverse Total Shoulder Replacement - Ben will recommend a reverse shoulder replacement when severe arthritis occurs together with a large rotator cuff tear.
In this procedure, the normal ball-and-socket structure of the shoulder is reversed. The ball component is attached to the shoulder blade, and the socket component is attached to the upper arm bone.
This design allows the larger deltoid muscle to lift the arm instead of the damaged rotator cuff tendons. Reverse shoulder replacement can provide excellent pain relief and improved arm function in patients with cuff tear arthropathy or complex shoulder problems.
Shoulder Fusion (Arthrodesis) - Shoulder fusion is rarely required but may occasionally be considered in younger patients with severe arthritis who are not suitable for joint replacement surgery.
During this procedure, the joint surfaces are fused together so the shoulder no longer moves. This eliminates the painful joint surfaces rubbing against each other and can provide reliable pain relief and stability.
Although shoulder movement is lost, patients are still able to use their shoulder blade and arm for some functional activities.
-
Ben operates at multiple hospitals across Melbourne’s bayside and peninsula region, including:
Linacre Private Hospital, Hampton
Peninsula Private Hospital, Langwarrin
Beleura Private Hospital, Mornington
He can discuss your preferences in person during your consultation.
-
Ben will see you for a post-operative appointment usually 2 weeks after your surgery. During this appointment he will asses your wound and check that healing and mobility is progressing as expected. There will be no cost for this appointment.
As well as this, Ben will usually refer you to a physiotherapist, who focuses on rehabilitation after an injury, and will work with you to improve function of the affected area.
-
You can usually start driving again 4-6 weeks after the operation. However, every surgery is different, so Ben will provide individualised advice as part of the initial consultation.