

Rotator Cuff Injuries
What is a rotator cuff tear?
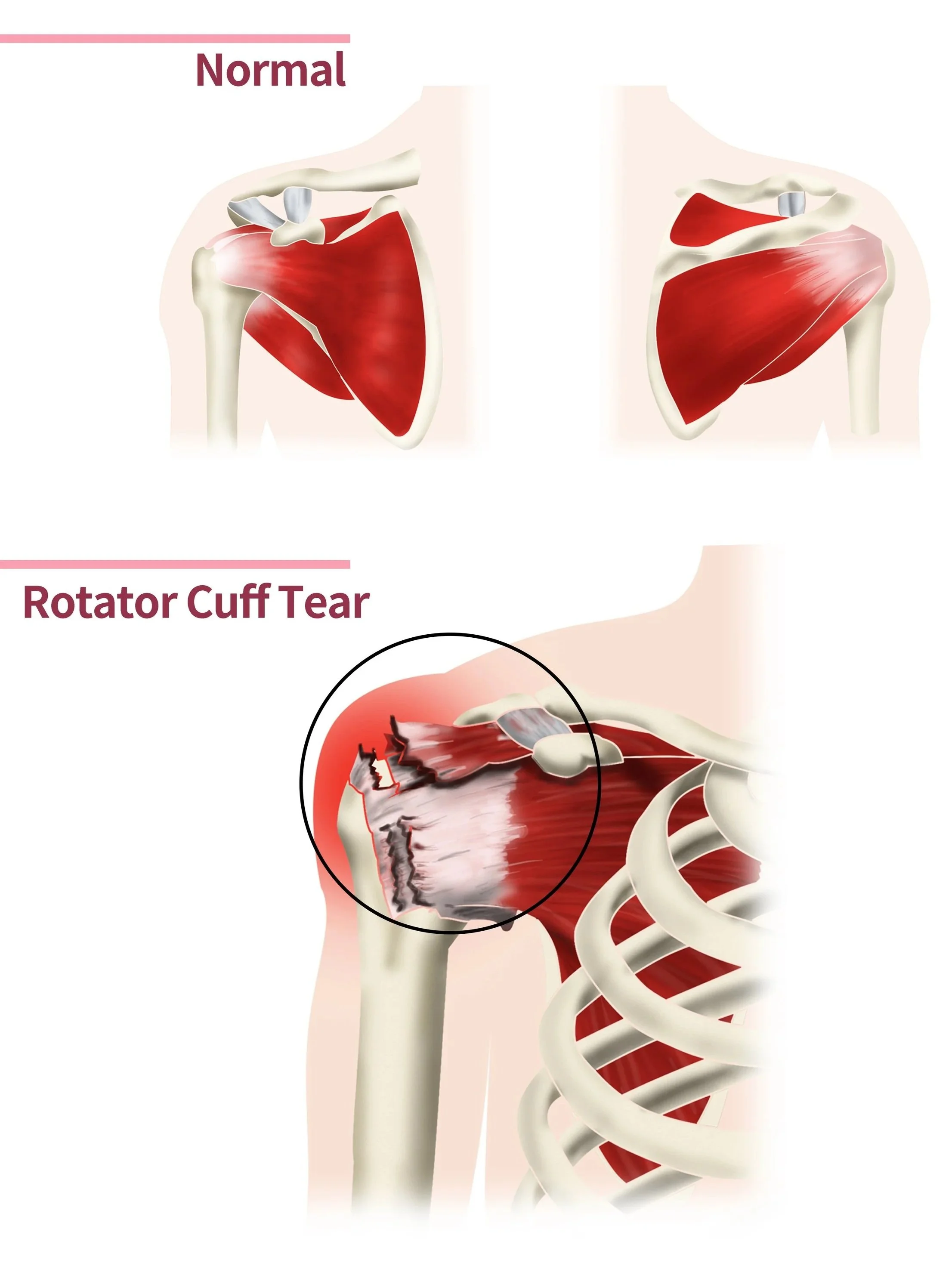
The rotator cuff is a group of four muscles and tendons that surround the shoulder joint and help keep the shoulder stable while allowing you to lift and rotate your arm. A rotator cuff injury occurs when one or more of these tendons become inflamed, damaged, or torn.
Rotator cuff tears can occur suddenly after a fall or heavy lifting injury, or they may develop gradually over time due to wear and tear. Degenerative tears are more common with increasing age and are often associated with repetitive overhead activities, heavy manual work, or long-standing shoulder impingement.
Rotator cuff injuries range from partial tears, where the tendon is damaged but still attached, to full-thickness tears, where the tendon completely detaches from the bone.
How do I know if I have a rotator cuff tear?
Rotator cuff injuries commonly cause pain around the shoulder and upper arm. The pain is often worse when lifting the arm overhead, reaching behind the back, or lying on the affected shoulder at night.
Common symptoms include:
Shoulder pain, particularly with movement
Weakness when lifting or rotating the arm
Difficulty reaching overhead
Pain at night or disturbed sleep
Clicking, catching, or cracking sensations in the shoulder
Reduced range of motion
Difficulty performing daily activities such as dressing or lifting objects
Some people notice a sudden tearing sensation after an injury, while others develop symptoms gradually over many months.
How Ben can help?
Diagnosing rotator cuff tears
Ben will begin by discussing your symptoms, medical history, and any previous injuries. During the examination, your shoulder movement, strength, and areas of tenderness will be assessed. Specific clinical tests may be performed to determine which rotator cuff tendon is involved and whether weakness or instability is present. Ben will often also arrange imaging investigations to confirm the diagnosis and assess the severity of the injury. These may include:
X-rays to assess the bones and look for arthritis or bone spurs
Ultrasound to evaluate the tendons dynamically
MRI scans to provide detailed images of the rotator cuff tendons, muscles, and surrounding structures
These investigations help determine whether the tear is partial or complete and guide treatment recommendations.
Treating rotator cuff tears
Non-surgical treatment
Many rotator cuff injuries can initially be managed without surgery, particularly partial tears or degenerative injuries with manageable symptoms.
Non-surgical treatment may include activity modification, rest, anti-inflammatory medication, and physiotherapy to improve shoulder strength and movement. A structured rehabilitation program can help restore shoulder function and reduce pain.
Corticosteroid injections may also be considered to reduce inflammation and provide temporary pain relief, particularly when pain is limiting rehabilitation.
Some patients achieve good long-term symptom control without surgery, although weakness or discomfort may persist in larger tears.
Surgical treatment
Ben will usually recommend surgery if non-surgical treatments have failed to provide pain relief, when there is significant weakness or loss of function, or following an acute traumatic tear in active patients.
There are a number of surgical options:
Arthroscopic Rotator Cuff Repair: This is the most common procedure used to treat rotator cuff tears. The surgery is performed through several small incisions using a camera and specialised instruments. The torn tendon is reattached back to the bone using sutures and small anchors inserted into the humerus.
Arthroscopic surgery allows treatment of associated problems within the shoulder, including bone spurs, inflammation, or biceps tendon pathology, while minimising damage to surrounding tissues.
Open Rotator Cuff Repair: In some larger or more complex tears, an open repair may be required. This involves a larger incision over the shoulder to allow direct access to the torn tendon. The tendon is repaired back to the bone using sutures and anchors in a similar way to arthroscopic surgery.
Ben will usually recommend an open repair if the tear is particularly large or the surgery is being revised.
Tendon Transfer Surgery: For severe or irreparable rotator cuff tears where the tendon cannot be repaired directly, a tendon transfer procedure may be considered. In this surgery, a nearby tendon is moved and attached to restore shoulder movement and function.
This option is usually reserved for younger or more active patients with significant weakness and preserved joint cartilage.
Reverse Shoulder Replacement: In patients with massive irreparable rotator cuff tears combined with advanced shoulder arthritis, a reverse shoulder replacement may be recommended. This procedure replaces the damaged joint surfaces and changes the mechanics of the shoulder so that other muscles can compensate for the deficient rotator cuff.
Reverse shoulder replacement can provide significant pain relief and improved shoulder function in appropriately selected patients.
Following surgery, the arm is usually supported in a sling for several weeks while the tendon heals. Physiotherapy and rehabilitation are essential parts of recovery, with gradual progression of movement and strengthening exercises over several months.
-
Ben operates at multiple hospitals across Melbourne’s bayside and peninsula region, including:
Linacre Private Hospital, Hampton
Peninsula Private Hospital, Langwarrin
Beleura Private Hospital, Mornington
He can discuss your preferences in person during your consultation.
-
Ben will see you for a post-operative appointment usually 2 weeks after your surgery. During this appointment he will asses your wound and check that healing and mobility is progressing as expected. There will be no cost for this appointment.
As well as this, Ben will usually refer you to a physiotherapist, who focuses on rehabilitation after an injury, and will work with you to improve function of the affected area.
-
You can usually start driving again 4-6 weeks after the operation. However, every surgery is different, so Ben will provide individualised advice as part of the initial consultation.