

Frozen shoulder
What is frozen shoulder?
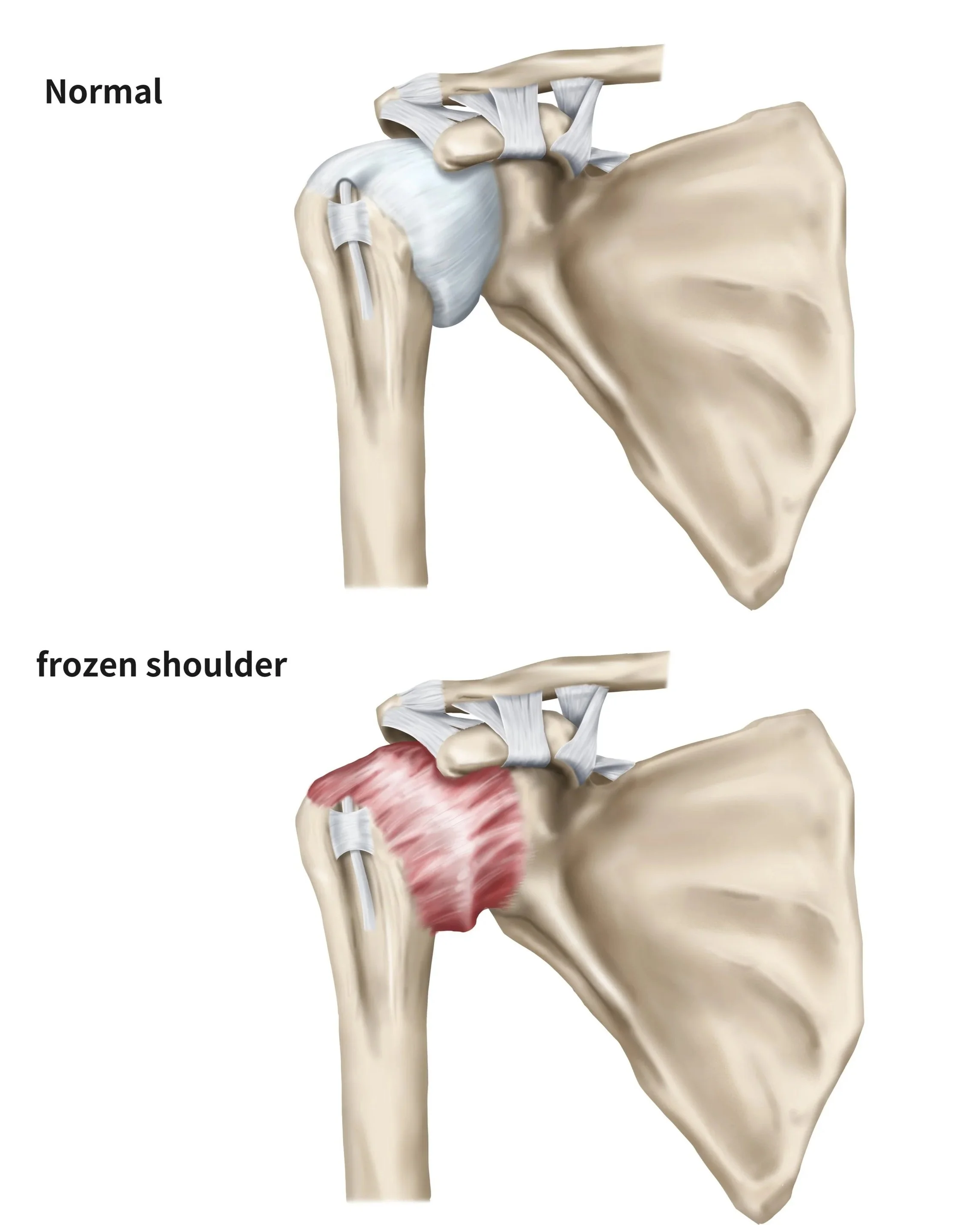
Frozen shoulder, also known as adhesive capsulitis, is a condition that causes pain and stiffness in the shoulder joint. It occurs when the capsule surrounding the shoulder becomes inflamed, thickened, and tight, leading to restricted movement and pain.
Frozen shoulder usually develops gradually over time and often progresses through three stages: a painful “freezing” stage, a stiff “frozen” stage, and finally a “thawing” stage where movement slowly improves.
The condition is most common in people between 40 and 60 years of age and occurs more frequently in women. It is also more common in people with diabetes, thyroid disease, Parkinson’s disease, and following periods of shoulder immobilisation after injury or surgery.
How do I know if I have a frozen shoulder?
The main symptoms of frozen shoulder are pain and progressive loss of shoulder movement. Both active movement (when you move the arm yourself) and passive movement (when someone else moves the arm for you) become restricted.
Common symptoms include:
Gradually worsening shoulder pain
Stiffness and loss of shoulder movement
Difficulty reaching overhead or behind the back
Pain that is often worse at night
Difficulty dressing, grooming, or performing daily activities
Reduced ability to lift or rotate the arm
Symptoms often develop slowly over several months and may continue for one to three years before improving.
How Ben can help?
Diagnosing frozen shoulder
Ben will discuss your symptoms, medical history, and any previous injuries or surgeries affecting the shoulder. During the examination, the range of motion of the shoulder is carefully assessed. A key feature of frozen shoulder is restriction in both active and passive movement, particularly external rotation.
Imaging tests are often ordered to exclude other causes of shoulder pain and stiffness. These may include:
X-rays to assess for arthritis or other bone abnormalities
Ultrasound to evaluate the rotator cuff tendons
MRI scans if other shoulder conditions are suspected
Although imaging may appear relatively normal in frozen shoulder, these investigations help confirm the diagnosis and rule out alternative problems.
Treating frozen shoulder
Non-surgical treatment
Most cases of frozen shoulder improve over time without surgery, although recovery can be slow. The aim of treatment is to reduce pain and gradually restore shoulder movement.
Non-surgical treatment may include anti-inflammatory medication, activity modification, and physiotherapy focusing on gentle stretching and range-of-motion exercises. A home exercise program is often an important part of recovery.
Corticosteroid injections into the shoulder joint may help reduce inflammation and pain, particularly during the painful early stages of the condition.
In some patients, symptoms gradually resolve over time, although mild stiffness may persist.
Surgical treatment
Ben will usually recommend surgery when symptoms remain severe despite prolonged non-surgical treatment, particularly when pain and stiffness significantly affect daily activities and quality of life.
There are a number of surgical options:
Manipulation Under Anaesthetic: During this procedure, the patient is placed under general anaesthetic and Ben will carefully move the shoulder through its range of motion to stretch and release the tightened capsule.
This procedure aims to improve shoulder mobility by breaking up scar tissue and adhesions within the joint.
Arthroscopic Capsular Release: This minimally invasive procedure is performed through small incisions using a camera and specialised instruments. The tight, thickened portions of the joint capsule are carefully released to restore movement.
Arthroscopic capsular release allows Ben to directly visualise the shoulder joint and address associated problems if present. It is commonly performed when significant stiffness persists despite physiotherapy and injections.
Combined Arthroscopic Release and Manipulation: In some cases, both arthroscopic capsular release and manipulation under anaesthetic are performed together to maximise restoration of shoulder movement.
Following surgery, physiotherapy is essential to maintain the improved range of motion and prevent stiffness from recurring. Rehabilitation usually begins soon after the procedure and continues for several weeks to months.
-
Ben operates at multiple hospitals across Melbourne’s bayside and peninsula region, including:
Linacre Private Hospital, Hampton
Peninsula Private Hospital, Langwarrin
Beleura Private Hospital, Mornington
He can discuss your preferences in person during your consultation.
-
Ben will see you for a post-operative appointment usually 2 weeks after your surgery. During this appointment he will asses your wound and check that healing and mobility is progressing as expected. There will be no cost for this appointment.
As well as this, Ben will usually refer you to a physiotherapist, who focuses on rehabilitation after an injury, and will work with you to improve function of the affected area.
-
You can usually start driving again 4-6 weeks after the operation. However, every surgery is different, so Ben will provide individualised advice as part of the initial consultation.